Plainly put, coarctation of aorta means the narrowing of the aorta. This generally happens at the level of the origin of the ductus arteriosus from the aorta. Ductus arteriosus is a part of the Fetal Circulation. After the birth, within a few days ductus arteriosus gets collapsed and fibrosed, paving way to the adult circulation system. The closure is managed by the drop of Prostaglandin E. Which is a lipid compound that is physiologically active. Which means the secretion of prostaglandin from the fetus keeps the ductus patent.
When the neonatal prostaglandin levels drop after birth, degeneration of the ductus arteriosus is underway. Coarctation of aorta is usually timed within the timeframe of this phase in pediatric patients, usually 2-5 days after birth. You would be presented with a very sick child, usually severe with metabolic acidosis and heart failure and absent femoral pulses.
In neonates, surgical management is indicated soon after diagnosis, however the initial management is to give prostaglandin infusion to keep the ductus arteriosus open to buy time.
In adults, the diseases is less acute and often subclinical, It can occur at the point of origin of ductus as pediatric patients mentioned above, or distal or proximally to that point. There are distinct clinical features to identify the location of the coarctation. Normally, in the majority of the cases the coarctation happens distal to the origin of the subclavian artery, this can be seen when the blood pressure readings of the upper extremities are the same and higher than that of lower extremities and a radio femoral delay is noted. When the narrowing happens proximal to the origin of the subclavian artery blood pressure readings between the upper extremities themselves are significantly different. A radio radial delay is also present. In severe coarctation, claudication of the legs are present. Coarctation causes an outflow tract obstruction from the heart. Which gives rise to a mid late systolic murmur heard over the upper precordium or the back.
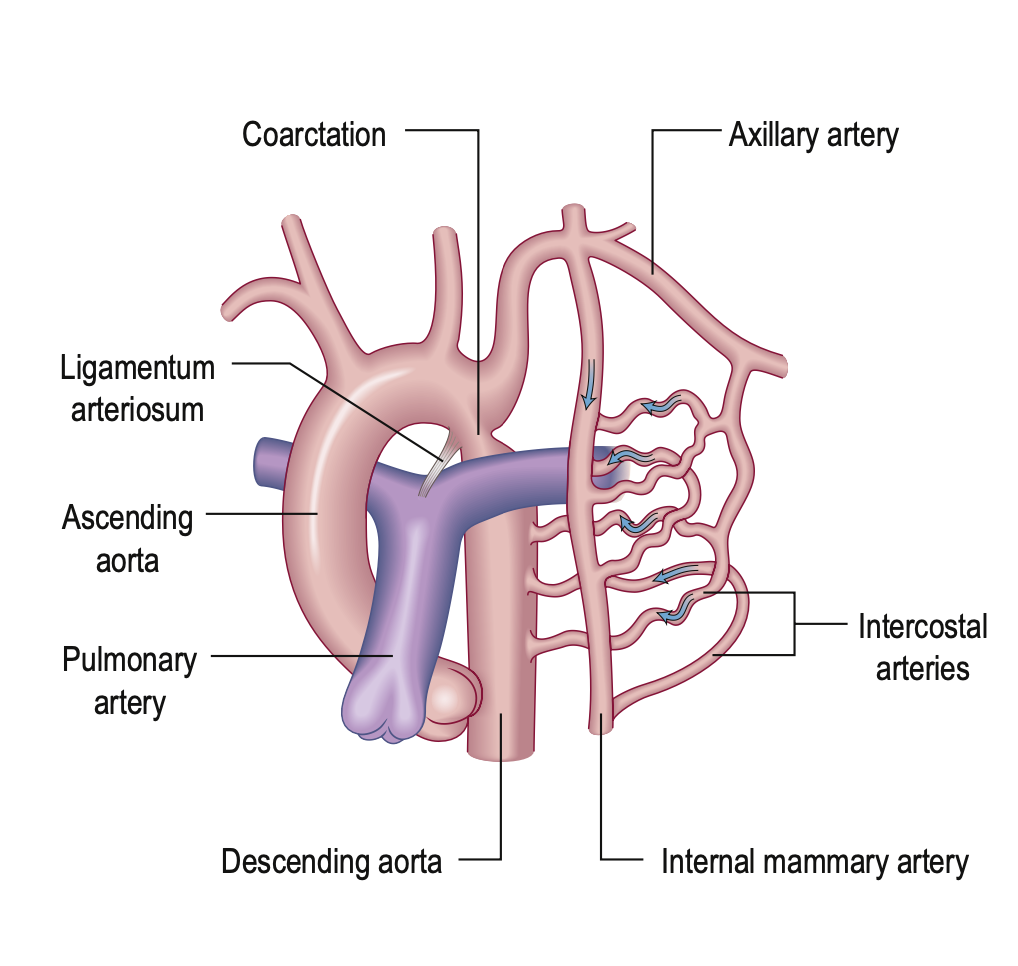
In adult patients with coarctation, circle of willis aneurysms may be present (10%). Severe narrowing of the aorta encourages the formation of a collateral arterial circulation involving the intercostal arteries. In 80% of adults with a coarctation a bicuspid aortic valve is seen.
The main chest X ray finding is the “3 sign” in the point of coarctation, Left ventricular hypertrophy in ECG. With MRI scanning the coarctation can be visualized with more detail.
Repair is indicated for adults only if the blood pressure difference is more than 20mmHg or if more than 50% of the lumen is narrowed. The preferred method is balloon dilation.
Sources: [1]:Kumar & Clark’s Clinical Medicine 10th Edition [2]: Illustrated Textbook of Pediatrics 4th Edition